
")
Carol Duff MSN, BA, RN
“The risk of melanoma seems to be increasing in people under 40, especially women” (Mayo Clinic, 2017). Melanomas are not the most common type of skin cancer, but they are the deadliest.
Skin cancer is the most common of all cancers and is also the easiest to cure if diagnosed and treated early. Self-examination is an important way to catch melanomas at their earliest stage of development.
Most people have between 10 and 45 moles. Usually normal moles are all one color, brown, black, or tan. They have a clear border, usually round or oval, that separates the mole from the surrounding skin. These moles are generally smaller than 6mm (1/4 inch), about the size of pencil eraser (Mayo Clinic, 2017).
The origins of melanoma
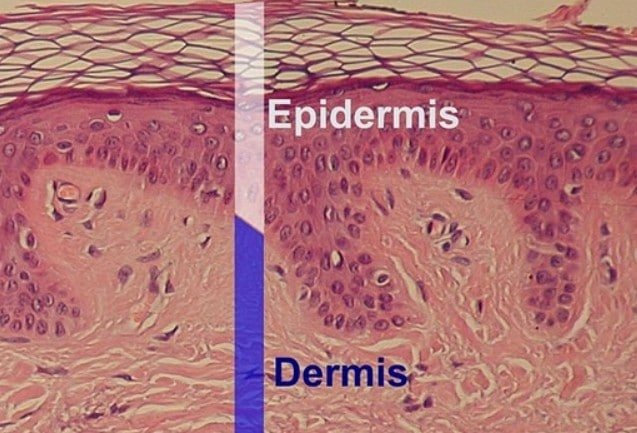
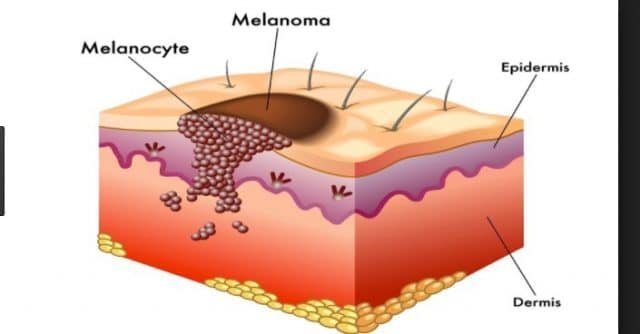
Normally the skin produces a protein called melanin made by melanocytes, which are located in the bottom layer of skin (dermis). Melanin gives your skin its color. The more melanin you have the darker your skin will be. Melanin absorbs ultraviolet (UV) radiation in response to exposure to the sun. The melanin tries to protect the skin by absorbing the UV radiation and produces a tan when the skin is exposed to sunlight. A melanoma may occur when there is uncontrolled growth (cancer) of the melanocytes of the skin.
People with dark brown or black skin have the same number of melanin producing cells, but produce more melanin and are less likely to have skin that is damaged by UV radiation. Non-cancerous growth of melanocytes produces moles and freckles. Cancerous growth of melanocytes produces melanoma. Malignant melanoma is responsible for over 1% of all cancer deaths.
New skin cells are constantly being formed and are pushing the old cells to the surface of the body to be shed. A melanoma (cancer of the pigment-producing cells of the skin) is really a cell growing without limit in a disorganized way, and in doing so is replacing normal tissues. Think of weeds overgrowing a vegetable garden. The DNA within the melanin cells has become disorganized, damaged and starts to grow too rapidly.
A melanoma starts on the surface of the skin, but if given time to grow may extend down into the skin and reach the blood and lymphatic systems and spread to other parts of the body and cause a life-threatening illness. While most melanomas will appear on areas of the skin that is regularly exposed to sunlight some can develop under the nails, on the soles of the feet, in the eye, on the mucous membranes of the mouth, intestines, or in the urinary bladder.

Melanoma often occurs in adults who are in the prime of their lives. Some traits and factors that can be associated with the incidence of melanoma are:
- Multiple moles
- Non-typical moles.
- Family tendency to have atypical moles.
- Disorders of natural repair of the skin.
- Too much exposure to the sun.
- Painful or blistering sunburn, especially when young.
- Living close to the equator or at high levels of elevation.
- Burns easily.
- Weakened immune system, such as someone who is on immunosuppressive drugs after receiving a transplant or being treated for autoimmune diseases.
- Unable to tan.
- Light hair and/or blue eyes.

Who Should Perform Skin Self Examinations?
Everyone. including children. who can be taught at an early age.
Skin examinations should be performed often and become a habit. Find a few moments at least every three months.

Where to look:
- The self-examination should start with the head and end with the feet.
- Self-examination should include the scalp, face, neck, beneath facial hair and trunk.
- On the upper part of the body, self-examination should include the armpits, hands including palms, finger webs, and nail beds.
- A mirror should be used to examine the back and skin between the buttocks.
- On the legs, which also should include toe webs, toe nail beds and soles of the feet.

If you are comfortable with having someone assist with areas it is difficult for you to see, please enlist their help in this process.
How does melanoma grow?
Genes control cell growth and melanoma is thought to be uncontrolled growth of the melanocytic stem cells with the eventual invasion into surrounding tissue. If the melanoma is only in the outer layer of skin (epidermis) this is called melanoma in situ and the cure is always excision of the questionable area because there is no potential spread to other parts of the body.
If the cancerous cells have penetrated deeper through the skin layers, this is called invasive melanoma. Once the melanoma cells have reached the lower layers of skin (dermis) there is a chance that the cancerous cells can spread by accessing the lymphatic system to the local lymph nodes or through the blood stream where is can reach organs such as the brain and lungs.
The chance of a secondary spread or further spread of the cancer (metastasis) depends on how deep the melanocytic cells have penetrated the skin. Early detection of melanoma will stop this spread of cells and is of utmost importance.

What are some of the risk factors for melanoma?
- Sun exposure, especially during childhood.
- Fair skin that burns easily.
- Blistering sunburn, especially when young.
- Previous melanoma.
- Previous non-melanoma skin cancer (basal cell carcinoma or squamous cell carcinoma.
- Family history of melanoma, especially if two or more members are affected.
- Large numbers of moles (especially if there are more than 100).
- Abnormal moles which are a larger size and/or have irregular borders.
Where do you look to find melanomas?
One half of the melanomas appear on normal looking skin or from a mole or freckle which starts to grow larger and changes in its appearance. Other lesions (abnormal areas of the skin) which can be the start of a melanoma are:
- Brown birthmark
- Strange looking mole
- Normal looking mole
Melanomas can appear anywhere on the body, not just areas that received sun exposure. For men, the back is the most common site and for women the most frequent site is the leg.

Melanoma usually start on the skin, but can grow on mucous membranes such as the lips and genitals. Sometimes a melanoma may grow on the eye, mouth, or vagina.
What does a melanoma look like?
- The first sign may be a changed or new freckle or mole.
- Unusual shape.
- May be seen when they are small at an early stage, but can grow much larger.
- May start as a flat area and then become raised.
- May have several colors including tan, dark brown, black, blue, red and sometimes light grey. There are melanomas that are the color of normal skin or are white or scarred in appearance.
- May or may not be itchy or be tender. More advanced areas will bleed easily and then crust over.
Although not all melanomas show these characteristics, there is a seven point checklist (Glascow) with major and minor features and also the ABCDE’s of melanoma.
Major Features:
- Change in size
- Irregular shape
- Irregular color
Minor Features:
- Diameter less than 7 mm (about one fourth of an inch)
- Inflammation
- Oozing
- Change in sensation
ABCDE’s of melanoma
- ASYMMETRY – one half unlike the other half
- BORDER IRREGULARITY-irregular, scalloped, or poorly defined border
- COLOR VARIATION-varied from one area to another: shades of tan and brown, black; sometimes white, red and blue.
- DIAMETER-over 6 mm or the size of a pencil eraser or can be smaller
- EVOLVING – enlarging, changing

Early detection requires some knowledge of what to look for and also some luck. Some melanomas may be the color of normal skin because they do not have pigment granules (which gives color). This is why it is important that any biopsy from your body be sent to a reputable dermatopathology laboratory for careful analysis. A lab of this category will have well-trained, Board-Certified Dermatopathologists.
As many as five percent of melanomas disappear after a period. It is now that they may have already spread into the body before a doctor can look at them. The disappearance of the loss of visible melanoma cells on the skin results from the body’s attempt to kill the melanoma cell with its own immune cells and antibodies.
As the body’s immune system attempts to kill the melanoma cells, the area of skin that surrounds the melanoma may also be killed and this produces the halo effect of a white ring around the melanoma.
If there is a diagnosis of melanoma, the doctor will examine the whole body to check if cancer cells have spread to other areas of the body such as nearby lymph glands. A careful exam of the skin will determine whether there are more suspicious areas of the skin.
Melanomas are surgically removed with the extent of the surgery depending on the thickness of the melanoma and where it is located. For thicker melanomas, the lymph glands near the melanoma area will be tested or removed.
What is Mole Mapping?
Mole mapping is a surveillance program for those who are at high risk of malignant melanoma. This may include a clinical skin examination and dermoscopy (close examination of the skin using skin surface microscopy to elevate pigmented skin lesions) to closely evaluate a suspected skin area.
Mole mapping may involve marking spots on a drawing of the body, print photographs, or digital images of the whole body’s skin surface. This mapping may be reviewed at a later date to see if there are new skin lesions or whether existing lesions have grown, changed color, or shape.
What is Digital Mole Mapping?

Sophisticated digital mole mapping may include:
- Risk evaluation (medical and family history, skin typing, sun exposure).
- Patient education about sun protection, moles, and melanoma.
- Skin examination by a professional (usually a doctor or specially trained nurse).
- High quality digital images.
- Poses of the whole body with areas of lesions of concern localized.
- Close-up images of the lesions of concern.
- Dermascopic images of lesions of concern.
- Evaluation of the images by an expert in skin cancer.
- A report to the patient and or referring health practitioner including suspected diagnoses and recommendations for treatment of lesions of concern.
- Follow-up mole mapping in three to six months for lesions of concern that are not ready for excision.
- Follow-up mole mapping of all imaged lesions at one or two-year intervals.
- A secure database and transfer system to store images and reports.
- Copies of images for the patient or doctor to aid self-skin examination.
Who is Suitable for mole mapping? Mole mapping is useful for those who have:
- Lots of moles (more than 50 to 100).
- Moles that are large, have an unusual color or shape.
- Moles on the back which are hard to keep track of.
- Strong family history of melanoma.
- Moles and fair skin which has been severely sunburned.
- Any concern about individual moles or freckles due to appearance or recent change.
Advantages of mole mapping:
- To diagnose melanoma at the earliest stage.
- Identify new lesions or changes in pre-existing lesions. The previous record can be used to determine whether a lesion is new or has changed.
- If the doctor decides that the lesions should be removed, this should be done at the earliest possible stage which will reduce the risk of melanoma and minimize surgery.
- If the lesion has changed or is new, but not necessarily at the threshold for removal, it can be re-imaged and watched carefully.
- Lesions which are not melanomas may not need to be removed, which will reduce the potential cost and complications of surgery.
- Digital mole mapping may be achieved near where you live.
- Earlier evaluation by an expert.
- Reassurance for the patient.
Risks of mole mapping:
- Mole mapping is a new procedure and is considered experimental by many dermatologists.
- There may be a melanoma in a site that has not been imaged (scalp, genitals.)
- A harmless lesion may be misdiagnosed as melanoma.
- Early melanoma may look like a normal mole and might really be positive for cancer.
- A melanoma may grow rapidly and may reach a dangerous size before the next scheduled visit for mole mapping.
- The procedure may be embarrassing.
Testing
Sometimes just looking at the suspected area of melanoma will not be enough to make an accurate diagnosis. You may need a biopsy which is removing a few cells for further examination in a laboratory. There are three types of biopsies:
- A punch biopsy is the use of a tool with a circular blade which produces a round section of skin from the suspected mole.
- An excisional biopsy is the removal of the entire mole along with what appears to be normal skin around the mole.
- An incisional biopsy which is the removal of the irregular part of the mole.
If the laboratory report confirms the diagnosis of melanoma the stage of seriousness of the melanoma will be determined with these methods:
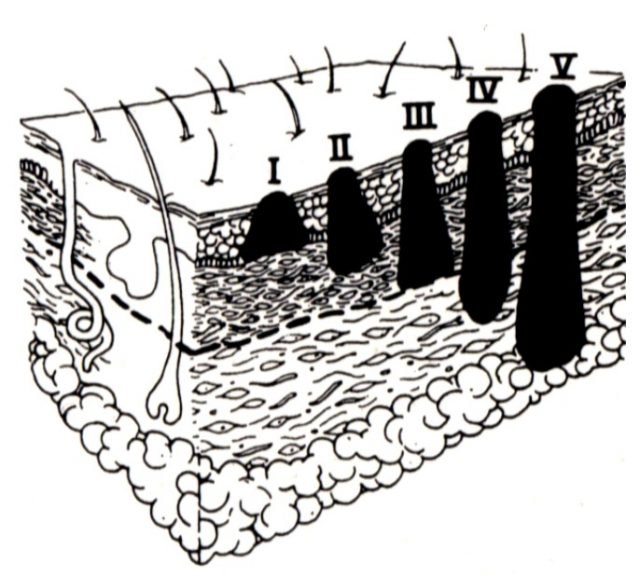
- Thickness of the tumor is measured by a micrometer in the laboratory. The thickness helps your doctor to decide on a treatment plan and generally, the thicker the tumor the more serious your disease.
- The second part of staging is to see if the melanoma as spread to surrounding tissues. Also, it will be determined whether parts of the melanoma have spread to the nearby lymph nodes using a process called sentinel node biopsy. Dye will be injected into the area from which the melanoma was removed and this dye will flow into the nearby lymph system/lymph nodes. If the first lymph node (sentinel node) has no cancer cells in it, chances are that the melanoma has not spread beyond the immediate area of removal. Note that cancer can still spread of recur even if the sentinel lymph nodes do not show cancer cells.
- The extent of the dividing cancer cells from the suspicious area are also looked at using a microscope. An open sore or an enormous number of dividing cancer cells will show the level of aggressiveness of the melanoma.
- The actual level of staging is represented by the Roman numerals I though IV. Stage I is small and has a promising treatment rate. The higher the staging number the lower the probabilities for a full recovery. With Stage IV the cancer has spread to other organs.

Treatment
Treatment depends on the staging (size and spread) of your melanoma.
Early stage melanoma will require the removal of the melanoma and enough surrounding tissue to exhibit that all portions of the melanoma have been removed.
Melanoma that has spread beyond the skin will require:
- Surgery to remove any affected lymph nodes.
- Chemotherapy in pill of intravenous form. Isolated limb perfusion is used if the melanoma is confined to an arm or leg. The blood which contains the chemotherapy fluid is only allowed to flow into the affected limb, avoiding traveling through the entire body. This process insures that the chemotherapy will not affect other parts of the body.
- Radiation therapy, to kill the cancer cells, may be used if melanoma has spread to lymph nodes.
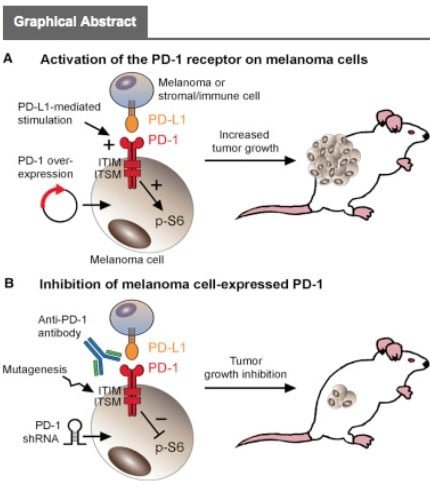
- Biological therapy which boosts the immune system to help fight the cancer. Biological therapies used to treat melanoma include interferon and interleukin-2, nivolumab (Opdivo), ipilimumab (Yervoy), and pembrolizumab (Keytruda).
- Targeted therapy is used to attack vulnerabilities in the cancer cells in treating advanced melanoma. These therapies are Vemurafenib (Zelboraf), trametinib (Mekinist), dabrafenib (Tafinlar). Your cancer cells must have a certain genetic mutation that will respond to these medications so the tumor will be tested for this trait.
Prevention
- Avoid the sun between 10:00 a.m. and 4:00 p.m. Remember that sun exposure over time will accumulate to cause skin changes.
- Sunscreens do not filter out all harmful UV radiation but the use of a broad-spectrum sunscreen with a SPF of at least 15, but preferably with an SPF of at least 30, broad-spectrum, water-resistant, is recommended by the American Academy of Dermatology. Apply every two hours and more frequently when swimming.
- Wear protective clothing. Some clothing types are labeled as photoprotective.
- Wear sun glasses which block UVA and UVB rays.
- NO tanning beds.
- Know your skin and notice changes.
References
American Academy of Dermatology (2009). Malignant Melanoma. Retrieved April 1, 2009. From http://www.aad.org/public/publications/pamphlets/sun_malignant.html.
American Cancer Society. https://www.cancer.org/cancer/melanoma-skin-cancer.html
Ignatavicius, D.& Workman, M. (2006). Medical-Surgical Nursing: Critical Thinking for Collaborative Care (5th edition). St. Louise, MO: Elsevier Saunders.
https://www.mayoclinic.org/diseases-conditions/melanoma/basics/definition/con-20026009. retrieved October 28, 2017.
Medicinenet.com. https://www.medicinenet.com/melanoma/article.htm
MedlinePlus. https://medlineplus.gov/melanoma.html
New Zealand Dermatological Society Incorporated (2009). Retrieved March 11, 2009 from http://dermnetnz.org/lesions/melanoma.html.
Silberman, Allan. Malignant Melanoma. Retrieved March 31, 2009 from http://www/cancernews.com/articles/melanomas/htm.
Skincancer.org. http://www.skincancer.org/skin-cancer-information/melanoma
Weber, Paul (1997). Melanoma, Malignant Melanoma. Retrieved April 1, 2009 from http://www.skincancerinfo.com/melanoma/melanoma.html

Carol graduated from Riverside White Cross School of Nursing in Columbus, Ohio and received her diploma as a registered nurse. She attended Bowling Green State University where she received a Bachelor of Arts Degree in History and Literature. She attended the University of Toledo, College of Nursing, and received a Master’s of Nursing Science Degree as an Educator.
She has traveled extensively, is a photographer, and writes on medical issues. Carol has three children RJ, Katherine, and Stephen – one daughter-in-law; Katie – two granddaughters; Isabella Marianna and Zoe Olivia – and one grandson, Alexander Paul. She also shares her life with her husband Gordon Duff, many cats, and two rescues.
ATTENTION READERS
We See The World From All Sides and Want YOU To Be Fully InformedIn fact, intentional disinformation is a disgraceful scourge in media today. So to assuage any possible errant incorrect information posted herein, we strongly encourage you to seek corroboration from other non-VT sources before forming an educated opinion.
About VT - Policies & Disclosures - Comment Policy



Comments are closed.